Case 1: A fifty-year-old male with a history of single-chamber (AAIR) pacemaker implantation for symptomatic sick sinus syndrome presented to the pacemaker clinic experiencing multiple episodes of dizziness. An electrocardiogram was taken(see the image). What is the most probable underlying diagnosis and probable aetiology??
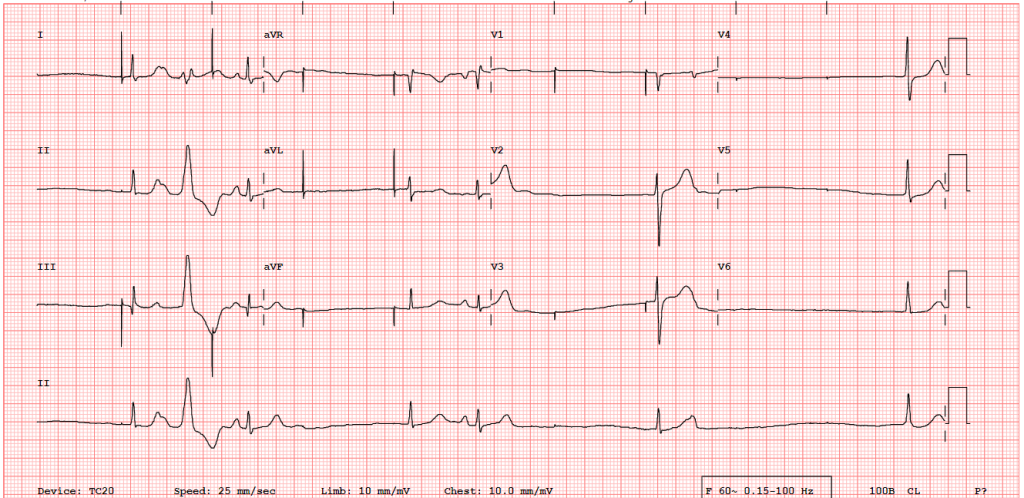
Figure 1. 12-lead electrocardiogram of the index patient.
Answer will be posted on the last week of June
Case courtesy: Dr Sudipta Mondal, SCTIMST, Trivandrum
Answer:
The electrocardiogram shows a lower atrial pacing rate of 60 per minute, and consistent atrial pacing at 1000ms intervals confirms no pacing failure . An absence of a P wave after an atrial pacing spike indicates failure of atrial lead capture (green arrows). While the 1st, 4th, and 6th QRS complexes may appear to be conducted beats after atrial capture, the lack of preceding P waves and morphological differences from true conducted ventricular complexes (as observed in the 3rd and 5th QRS complexes following intrinsic sinus P waves) definitively classify them as junctional escape beats. Additionally, the 2nd ventricular complex constitutes a ventricular premature complex (VPC). The electrocardiogram demonstrates an intrinsic P wave superimposed on the downslope of the T wave associated with the first QRS complex (indicated by the large arrow). This intrinsic P wave is followed by an atrial pacing spike approximately 520 milliseconds later. This temporal dissociation between the intrinsic P wave and the subsequent pacing spike confirms atrial lead sensing failure. This means the pacemaker failed to detect the intrinsic electrical activity of the atrium and delivered a pacing stimulus before the pre-programmed 1000 milliseconds delay, despite the presence of a native beat. Hence, he was diagnosed with sensing and capture failure.
Device interrogation showed a high impedance of >3000 Ω and a threshold of >7 Volts, even with a 1 millisecond pulse width, with rare erratic capture. Fluoroscopy confirmed a lead fracture at the junction of the pulse generator and the lead, with no dislodgment at the atrial side. He underwent lead revision, and he is doing well.
Pacemaker failure
Failure of pacing
Pacemaker failure
This ECG is showing intermittent spells of p pacing but without emerging
QRS – AV nodal blockade =the reason of syncope episodes even in the presence of AAIR pacing
This ECG is showing intermittent spells of atrial pacing but without corresponding emerging of QRS –AV node blockade.AAIR pacing is not suitable under such situation with SSS
Failure to pace and undersensing. Likely lead dislodgement
Pacemaker failure